

Background: Generally, DNA damage is counterbalanced by multiple pathways for DNA repair. However, by disturbances of this equilibrium, somatic cells accumulate mutations during development and aging. This increase has been implicated to be a major cause of not only aging but also of cancer development. Moreover, mutations in some genes (mainly DNMT3A, TET2, ASXL1) that are known to be present in patients with AML or MDS were also detected in individuals without hematological neoplasms (clonal hematopoiesis of indeterminate potential, CHIP) in an age-related manner.
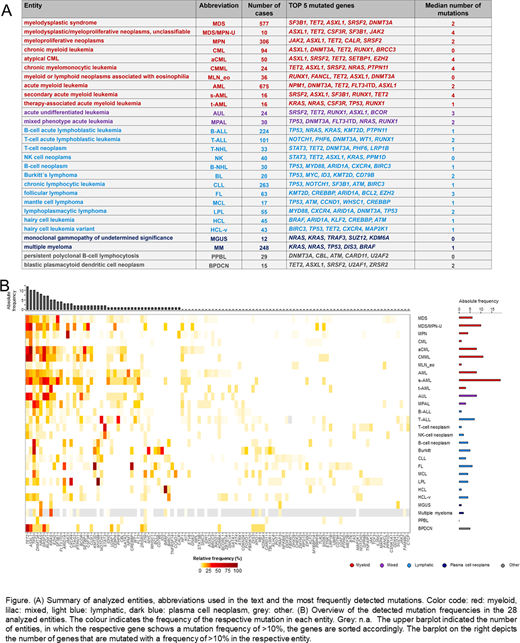
Aim: We correlated the mutation frequencies of 122 selected genes in 2656 cases with 11 different hematological malignancies (number of cases per entity ≥50 each) with age of the respective patients.
Methods: Whole-genome sequencing (WGS) was performed for all 2656 patients. For this, 151bp paired-end reads were generated on NovaSeq 6000 machines (Illumina, San Diego, CA). For correlation analysis, the Pearson correlation coefficient (bivariate correlation) was used (SPSS version 19.0.0 software, IBM Corporation, Armonk, NY). For comparison of median values, the independent samples t test was applied (SPSS). All reported p-values are two-sided and were considered significant at p<0.05.
Results: The age of the analyzed cohorts differed strongly, ranging from 37 years (median; range: 11 - 91 years) in T-ALL, 54 years (43 - 88) in FL and 54 years (0.1 - 93) in B-ALL to 73 years (23 - 93) in MDS and 74 years (50 - 92) in aCML. In the cohort of 2656 patients, totally 5709 mutations in the 122 analyzed genes were detected. A correlation of age with the numbers of mutations per patient was detected for the total cohort (median for patients ≤60 years: 1; >60 years: 2; p<0.001) and for AML (p<0.001), B-ALL (p=0.015), CLL (0.039), MDS (p<0.001), MPN (p<0.001) and T-ALL (p=0.005), but not for aCML, CML, FL, LPL and MM. This effect was less pronounced when CHIP-related genes (ASXL1, DNMT3A, TET2) were omitted from the cohort (total cohort: p=0.025; AML: 0.001; MDS: 0.001). When correlating the mutation frequencies with age, the strongest influence was found for AML, as 17 genes were significantly mutated in an age-related manner: mutations in KIT, POT1, RAD21, U2AF2 and WT1 were significantly correlated with younger age, whereas for ASXL1, BCOR, BCRR3, DNMT3A, ETV6, IDH2, RUNX1, SRSR2, TET2, TP53, U2AF1 and PHF6, a significant correlation with older age was observed. Of note, most mutations correlating with younger age were associated to an aberration known to occur itself in younger age, e.g. the vast majority of KIT mutations in AML were associated with t(8;21)(q22;q22)/RUNX1-RUNX1T1 or inv(16)(p13q22)/CBFB-MYH11 (22/25 cases, 88%), a similar observation was detected for RAD21 in AML (associated with t(8;21) in 8/19 cases, 42%). Age-dependent mutational profiles were also detected for CLL, B-ALL, MDS, MPN, T-ALL, FL, MM and LPL (see Table). No age-dependent differences in mutational patterns were detected for aCML and CML. The genes that were found to be mutated in most entities in older patients comprised TET2 (in 6 entities), TP53 (n=4), DNMT3A (n=3), ASXL1, BCOR, EZH2, GATA2 and IDH2 (n=2, respectively). By contrast, POT1 was found to be preferentially mutated in younger patients in 2 entities (AML and LPL). Moreover, for some mutations the relation to patient age was entity-specific: PHF6 mutations were correlated to younger age in CLL (median age mutated vs. unmutated: 43 years vs 67 years), but to older age in AML (74 vs. 68), similar to CD79B (older age: CLL, 93 vs. 67; younger age: LPL, 52 vs. 71) and NRAS (older age: T-ALL, 75 vs. 34, younger age: AML, 63 vs. 69, and MM, 65 vs. 70). Interestingly, all of the age-correlations that were detected recurrently remain even if CHIP-related genes were omitted from the cohort.
Conclusions: (1) A number of mutations were found to be correlated to older age across entites, comprising CHIP-related (TET2, DNMT3A, ASXL1) but also other genes (e.g. TP53, EZH2, BCOR, GATA2, IDH2). These correlations were found to be independent of the presence of CHIP-related mutations. (2) A lower number of mutations was correlated with younger age and associated with other age-related aberrations. (3) Some mutations show varying age-relation dependent on the entity, e.g. PHF6 mutations (CLL, younger age; AML, older age; T-ALL, equal distribution), proposing differences in mutation mechanisms or selection dependent on the respective entitiy.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal